Blocked Tear Ducts – Adults Dacryocystorhinostomy (DCR)
What Is a Tear Drain and How Does It Work?
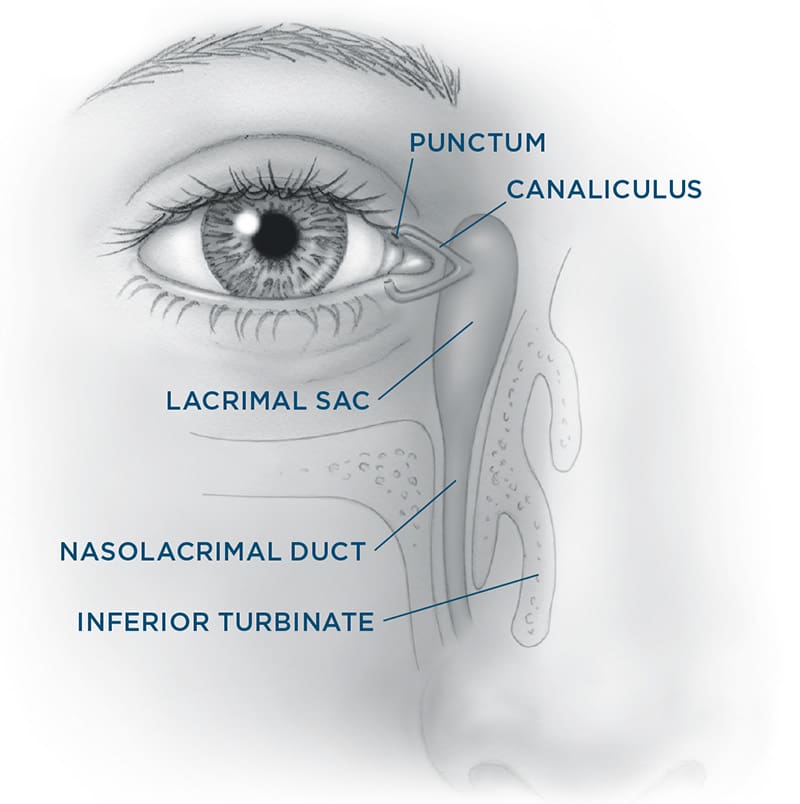
Tears normally drain through a small system that starts with two tiny openings — one in your upper eyelid and one in your lower eyelid, near the inner corner of your eye. These are called puncta. Tears pass from the puncta into small channels (canaliculi), then into a sac between your eye and nose (lacrimal sac), and finally through a duct (nasolacrimal duct) into your nose.
Every time you blink, this system pumps old tears away from the eye and into the nose, helping to keep your eyes moist and clear.
What Happens When It’s Blocked?
If the drainage system becomes blocked or narrowed, tears back up. This can lead to:
• Excessive tearing (watery eyes)
• Mucus buildup in the inner corner of the eye or lashes
• Blurry or distorted vision
• Swelling, tenderness, or redness near the inside corner of the eye
Your oculofacial plastic surgeon can usually determine where the blockage is and recommend the best treatment.
Treatment Options
Non-Surgical Options
Some cases may be treated with:
• Warm compresses
• Antibiotic drops
• Minor office procedures to open the puncta or small channels
Surgical Options
In most adults, a DCR (dacryocystorhinostomy) is the standard surgery to fix a blocked tear duct.
In a DCR:
• A new drainage opening is created between the tear sac and the inside of the nose, bypassing the blocked duct.
• A soft silicone stent may be placed temporarily to keep the passage open during healing.
• The surgery can be done through a small skin incision or inside the nose.
• It’s usually an outpatient procedure, done with either twilight sedation or general anesthesia.
• Most people recover in a few days, though mild nosebleeds and bruising are common.
If the blockage is in a less common location — like the canaliculus — your surgeon may recommend a different surgery called a CDCR (conjunctivodacryocystorhinostomy). In this case, a small glass tube (Jones tube) is used to drain the tears. These tubes may require more maintenance, including cleaning or replacement over time.
Risks and Complications
As with any surgery, there are some risks:
• Bruising and swelling between the eye and nose (usually goes away in 1–2 weeks)
• Bleeding or infection
• Scarring or narrowing of the new drainage passage over time
• A second procedure may be needed if tearing continues
If you use a CPAP machine for sleep apnea, let your surgeon know. After tear drain surgery, some patients feel air from the device around their eye.
Your surgeon will explain what to expect and how to care for the area after surgery. While most people improve, no surgery can guarantee perfect results.
Summary
Blocked tear ducts in adults can cause constant tearing, irritation, and even infection. A DCR is the most effective surgical solution for many cases. Most people see significant improvement after treatment. Your oculofacial plastic surgeon will help you choose the right option based on your specific condition.